Revolutionizing Cardiovascular Therapy: The New Insights on Beta Blockers
In the late 1950s, Sir James Black pioneered a groundbreaking advancement in cardiovascular therapy with the introduction of beta blockers . This class of medication quickly became a cornerstone in the management of patients with acute myocardial infarction , improving survival rates and reducing mortality significantly. However, recent studies have emerged, challenging long-held beliefs surrounding their use and suggesting that the administration of beta blockers may not be necessary for all patient profiles.
Rethinking the Necessity of Beta Blockers
A significant body of research, published in reputable medical journals, has presented a more nuanced view on the administration of beta blockers. Notably , patients with specific clinical profiles—particularly women—may not require these medications after an acute myocardial infarction if certain conditions are met. This calls for a more personalized approach in cardiac care.
The Historical Context of Beta Blockers
To grasp the significance of these recent findings, it is essential to travel back to the 1980s , when the foundational studies endorsing beta blockers were conducted. At that point in time, heart attacks were managed very differently. There were fewer interventions available, such as urgent angioplasties or the wide use of high-potency statins . In this landscape, beta blockers were shown to reduce mortality by an impressive 23%, making them indispensable in acute care.
The Current Challenge
In today’s landscape, the standard treatment for heart attacks has evolved significantly. Consequently, a pertinent question arises: Are beta blockers still universally necessary for all patients, particularly those whose hearts remain relatively intact post-infarction?
Understanding Left Ventricular Ejection Fraction (LVEF)
To appreciate the implications of this new research, one must understand left ventricular ejection fraction (LVEF) . This metric measures the percentage of blood the heart pumps out of the left ventricle with each contraction. Clinically, two main scenarios are considered:
- Patients with a reduced LVEF (≤40%): This indicates a weakened heart, and it is widely accepted that beta blockers are beneficial in this group due to solid evidence.
- Patients with a non-reduced LVEF (>40%): The heart retains good function, and here lies the crux of the debate on the necessity of beta blockers.
The REBOOT Trial: A Paradigm Shift
The REBOOT trial , an extensive study conducted in Spain and Italy, involved over 8,500 patients who suffered acute myocardial infarctions but had LVEF over 40%. Participants were divided into two groups—one receiving beta blockers and the other not.
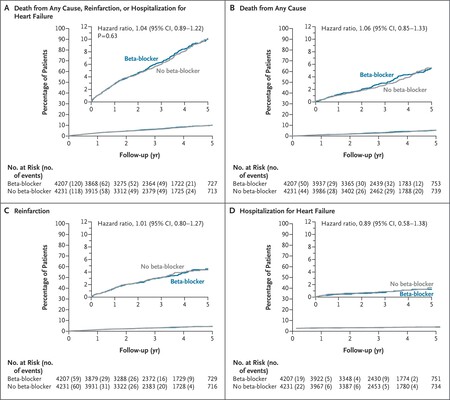
After a follow-up period averaging 3.7 years , the results were remarkable: there was no statistically significant difference in outcomes between the two groups. The event rate for both groups was nearly identical, leading to a conclusion that the traditional need for beta blockers could be questioned, particularly for specific populations.
Gender Differences in Beta Blocker Efficacy
Analyzing the REBOOT data by sex revealed intriguing patterns. Among the 1,627 women in the study, those who took beta blockers experienced a 45% higher relative risk of encountering significant health events compared to those who did not. This compelling finding warrants further research into the pharmacokinetics of beta blockers in women.
Compounding the Complexity: Conflicting Studies
As is often the case in medical research, the landscape is layered with complexity. Studies like Betami and Danblock , conducted in Norway and Denmark with nearly 5,600 participants, drew contrasting conclusions. They found that beta blockers did confer benefits, significantly lowering the risk of primary health events and new myocardial infarctions.
A Meta-Analysis: Seeking Consensus
In light of varying results, an international team of researchers conducted a meta-analysis combining data from the REBOOT, Betami, Danblock, and another smaller study. This analysis focused on patients with slightly reduced LVEF (40%-49%), categorizing them as a “gray area” for prognostic benefit.
Conclusion: Navigating the New Paradigm
The analysis concluded that in this specific group, beta blockers are indeed beneficial, reducing risk by 25% for heart attacks and heart failure. This indicates a nuanced understanding of when beta blockers optimize patient care. As such, cardiologists are urged to evaluate treatment on an individual basis. While beta blockers remain crucial for patients with significant heart damage, care should be tailored accordingly for those with preserved heart function. As more studies emerge, it is vital for healthcare providers to stay vigilant and informed, adjusting their treatment protocols based on the most recent evidence.
Images | Ali Hajiluyi, Towfiqui Barbhuiya